The Prodrome to Delirium
 A Grounded Theory Study
A Grounded Theory Study
Journal of Hospice and Palliative Nursing. 2013;15(6):332-337.
Abstract and Introduction
Abstract
Delirium is a state of confusion that occurs in up to 90% of patients
facing end-of-life. Despite its prevalence, there is a paucity of data
that describes the prodrome to delirium. Family and caregivers are key
observers of the phenomenology of delirium and often recall subtle signs
and symptoms that herald the delirious episode. The objective of this
study was to describe caregiver observations regarding the onset,
characteristics, and progression of the predelirium state in hospice
patients diagnosed with delirium. A purposive sample of 10 caregivers of
hospice patients took part in private, semistructured, audiotaped
interviews. The interviews were transcribed verbatim and analyzed using
the Straussian approach to grounded theory.
Six categories of
commonalities emerged:
physically declining,
cognitively/psychologically
declining,
withdrawing, end-of-life awareness,
deteriorating sleep
pattern,
and suffering.
A process model was created that illustrates the
temporal progression of sleep deterioration in the presence of overall
decline, which leads to the diagnosis of delirium.
In addition, the
model illustrates the experience of suffering, which is woven throughout
this temporal decline, becoming increasingly magnified as delirium
progresses.
These findings provide insight regarding early signs and
symptoms of emerging delirium.
Methods
Study Design
The current study was based on grounded theory methodology, which
provides insight into complex processes and significant life events such
as delirium in the dying patient using inductive methods to analyze
qualitative data.[23] Corbin and Strauss[24]
noted that grounded theory development involves the discovery of
concepts and recognition of themes within data and identifying
relationships between themes and categories derived directly from the
data and not from preconceived hypotheses. The Straussian method
incorporates a current literature search as well as the researchers'
previous experiences with the topic in question and offers a transparent
and structured method for exploring otherwise elusive details and
processes.[25,26]
The study was reviewed and approved by the Center for Hospice &
Palliative Care's Proposal Review Committee as well as the Daemen
College Human Subjects Research Review Committee. Written consent was
obtained from each participant who voluntarily took part in the study.
Participant interviews were conducted over a 3-month period in 2012. The
data used in this study were a subset of data collected for a larger
study, which looked at the progression of delirium in advanced illness
from both the caregiver and clinician perspective.[27]
Participants
Study participants included a purposive sample of caregivers of
hospice patients admitted into the Hospice Buffalo Inpatient Unit with a
diagnosis of delirium according to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition
criteria. To be included in this study, caregiver participants had to
be 18 years or older, English-speaking, and willing to talk with the
researcher in an interview format about their observations regarding the
onset, features, and course of witnessed clinical progression toward
delirium. Patients with a history of psychosis or thought disorder,
diagnosis of dementia, encephalopathy, brain metastasis, or signs of
significant renal or hepatic dysfunction were excluded from this study
as these factors may produce many of the same symptoms seen in delirious
patients.
Procedures
Consenting caregivers participated in a semistructured interview with
open-ended questions regarding observations of their loved ones in the
period prior to admission to the Hospice Buffalo Inpatient Unit. Each
interview was between 20 and 45 minutes in length, audiotaped, and
transcribed verbatim without identifying information in order to
maintain confidentiality in preparation for analysis. The data analysis
process included open, axial, and selective coding, which entails
identifying and assigning labels to what is happening in the data,
relating and categorizing those labels, and then selecting which
categories and relationships are the central processes to the developing
theory, thus ensuring that the theory is grounded in the data.[24]
To ensure a high level of validity and rigor, two independent
researchers manually coded all data. In addition, to determine fit of
findings after theoretical saturation of the major categories was
reached, the emerging theory findings were brought back to participants
to determine that they accurately reflected their experience of the
prodrome to delirium. Theoretical saturation, the point at which no new
significant relationships or characteristics regarding the emerging
theory are identified, was reached after interviewing 10 participants.
Introduction
Delirium is a complex syndrome with multiple etiologies characterized
by fluctuating disturbances in consciousness, attention, memory,
thought, and perception.[1–3]
Delirium is nearly ubiquitous within medical settings and is the most
common psychiatric disorder among the cancer patient population.[4–6]
It is present in most patients at the end of life, associated with
poorer survival, and is an independent predictor of mortality.[7–12]
Despite the prevalence and significance of delirium, it remains underdiagnosed and undertreated.[5,13–15]
Delirium can accelerate the end-of-life process, despite being potentially reversible in as many as 50% of cases.[16,17]
In part, inconsistent assessment and diagnosis may limit the
clinician's ability to recognize the underlying pathogenesis of
delirium.[7]
Unfortunately, delirium is often not diagnosed until in its fulminate
state, and there is a paucity of data that describes or detect the
prodromal phase of delirium.[7,12,16,17]
There is a need for studies that clarify the risk factors and
pathogenesis of delirium in order to provide earlier detection, prevent
further worsening in reversible cases, and provide a strategy that
reduces the risk of developing delirium.[18]
Although delirium in certain cases may be linked to specific
etiologies, such as infection, sleep disturbance, medications,
dehydration, urinary retention, pain, or constipation,[1,3] many delirious patients have no clear toxic or metabolic abnormality.[19] A more complete description may require acknowledgement of less definable causes or contributing factors.
Family and caregivers are key observers to the phenomenology of
delirium and often recall subtle signs and symptoms that herald
delirious episodes.[14,20–22]
They are often witness to the earliest manifestations and challenges of
delirium, such as nocturnal agitation and behavioral disturbances, and
may score even higher than their delirious loved ones on measures of
distress.[2]
Caregivers therefore are in the best position to alert health care
providers to early signs and symptoms of delirium. The caregiver
perspective also highlights the fact that delirium has impact beyond the
patient and is a source of suffering for caregivers as well as their
loved ones.
The purposes of this study were to explore the development and
progression of delirium experienced by hospice patients and to generate a
theoretical model that describes the prodrome to delirium as observed
by caregivers. Grounded theory analysis was used to establish categories
and characterize the progression of observed patient changes leading to
the development of delirium in an effort to more clearly define the
prodromal phase of delirium.
Results
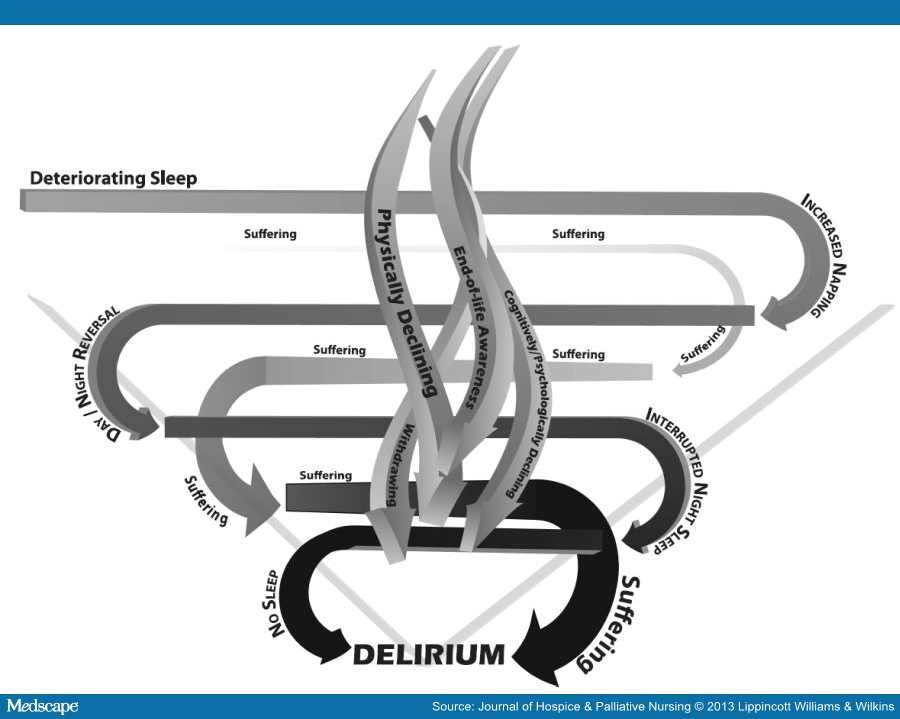
Ten caregiver participants were interviewed regarding changes observed in their loved ones during the time period leading up to the diagnosis of delirium. This time period varied greatly among participants. Some reflected back over a period of months, whereas others offered their observations of change and decline over a period of days to weeks. Despite variations in preceding timeframe, participants overwhelmingly described suffering, the core category that emerged in this study, as the process that encapsulated all other processes. Those other processes included physically declining, cognitively/psychologically declining, withdrawing, end-of-life awareness, and deteriorating sleep pattern. A theoretical model depicting this process is presented in the Figure. This model shows the overall patterning of the processes that occurs in the time preceding outright delirium; whether the processes occurred gradually, stepwise, or suddenly was variable between patients and may be due to factors such as differences in underlying etiologies. This model depicts a V-shaped frame representing the decreasing fullness of life, which ultimately ends in delirium, depicted in bold letters at the bottom point of the V-frame. Centralized, interwoven, downward spiraling arrows represent 4 of the 6 processes leading to delirium (physically declining, cognitively/psychologically declining, withdrawing, and end-of-life awareness) that are experienced by most patients, although there was wide variation in degree and no pattern noted other than an overall decline (Figure). Conversely, the fifth category, deteriorating sleep pattern, was prominently noted in all caregiver interviews and is depicted by an arrow that winds through and around the entire process leading to delirium. The ribbon intensifies from light to dark, depicting the progressive deterioration of sleep and the severity of its impact on patients. Similarly, a ribbon winding through the entire figure and intensifying in relationship to disrupted sleep depicts the core category of suffering. Descriptions of each category are listed below.
Process model of delirium.
Physically Declining
Participants reported a range of physical changes in their loved ones, including increased pain, decreased appetite, difficulty breathing, and generalized weakness. Physical weakness and falls were frequently reported. Examples included "he kept falling down," "2 weeks ago he could walk with a walker and now he can't even stand up," "she could hardly walk at all," "she went limp," "he didn't have steady legs anymore," and "she was too weak to sit up." Other observations regarding physical change were reported: "I think he was in pain," "her coloring changed," "she would not eat," and "her biggest problem was breathing."Cognitively/Psychologically Declining
Participants observed changes in their loved ones that involved cognition, personality, and behavior. Examples of the latter included "he yells at me," "she was going to hit me," "she gets mad and tells me to shut up," "she talks vulgar," "I noticed irritability and agitation," "he was screaming 'get me out of here,'" and "he twisted my daughter's arm and punched an aide." Participants noted cognitive changes such as memory loss and confusion. Examples included "he forgets right away" and "she had no idea who we are." Disorientation was frequent with one caregiver describing her loved one repeatedly asking what time it was even though he was sitting in front of a clock. Disorders of thought were reported, including perceptual disturbances. Examples of such observations included "she's been seeing people next to her" and "she kept thinking there was a policeman looking in all of the windows." Visual hallucinations involving insects, especially spiders, were prevalent. Others described emotional distress such as "fear" or restlessness such as pacing.Withdrawing
Participants described patient withdrawal in statements such as "nothing interested him anymore" and "I noticed she is not interested in things." One caregiver explained that her loved one used to live for visits from her grandchildren but now would not speak to them when they came to visit. Another participant explained that her loved one would no longer look at her favorite magazine. Inability to focus was commonly described: "she'd just stare ahead," "he'd just stare right through things," "he never really focused anymore," "she is not there in the moment," and "she'd just stare ahead when you are talking to her." One participant summed up her loved one's withdrawing by saying, "his eyes didn't shine anymore."End-of-Life Awareness
Issues surrounding end-of-life awareness evoked the greatest emotion from caregivers. Nearly all caregivers reported that their loved one expressed awareness of the dying process or impending death. One caregiver recalled that her loved one made comments such as "I wonder what it's like in the end" and "I wonder if I'll know when it's time." Another caregiver said her loved one stated "I'm dying… I feel it… there is a veil coming down over me." Others reported themes of life review and "going back over life events." One caregiver recounted her loved one's vivid funeral dream and noted that her loved one began to say goodbye, asking if the caregiver was going to be okay. Another of the caregivers described a "breakthrough moment" in which his previously confused loved one suddenly gained clarity, recognized everyone around him, hugged them, and expressed his love.Deteriorating Sleep Pattern
Disrupted sleep was the most commonly reported change observed by participants. Sleep fragmentation was described as frequent awakenings, alterations in the day/night cycle, and increased daytime somnolence. Participant reports included "he was always sleepy," "he was sleeping more," "she did sleep a lot more during the day than a normal person did," and "she would sleep 16 hours a day." The next reported change involved day/night reversal in which loved ones slept during the day, awoke in late evening, and often stayed awake all night. One participant recounted: "She would get up and have breakfast, and it wasn't even an hour later, and she would not say anything, and she would go back to bed and sleep for 3 to 4 hours and even past meal time, and I would go in and say 'do you want lunch,' and she would sleep past that and that would go on for 2 to 3 days most times. Then she would be up all night."Suffering
Suffering clearly emerged as the overarching process that defined the prodromal phase of delirium and was experienced by both participants and their loved ones. Statements included "I knew he was suffering, whether it was mentally or physically," "there is no question he is suffering—he is in a state of suffering," and "he was suffering, absolutely." Psychogenic suffering was inferred by participants who reported that their loved one was experiencing sadness, depression, frustration, and feeling as if they were "trapped." One participant recounted her loved one screaming "God… why are you doing this to me?" Throughout the interviews, participants struggled with their emotions, often crying as they reflected back upon these events.Discussion
The current study examined the onset, features, and progression of delirium in hospice patients as described by their caregivers. Given their special role, caregivers are often witness to the subtle signs and symptoms that precede delirious episodes.[14,20–22] Caregiver observations were analyzed using grounded theory methodology, which revealed six categories of clinical changes leading to the diagnosis of delirium: physically declining, cognitively/psychologically declining, withdrawing, end-of-life awareness, deteriorating sleep pattern, and suffering. Although the categories identified within this study have previously been associated with either delirium or the end-of-life process, there is an absence of data exploring the progression of signs and symptoms leading to the diagnosis of delirium.[7,16,17]Prior studies have established a connection between illness progression and delirium. Morita et al[21] surveyed bereaved family members whose loved ones developed delirium. Family members associated factors such as pain, medications, and physical discomfort with the emergence and progression of delirium.[21] Caregivers interviewed in this study also noted pain and generalized decline in the timeframe leading up to delirium. Physical weakness, to the point of falling down, was described in multiple interviews. This finding has not been previously explored in relationship to delirium and may warrant further consideration, as it is not clear whether falls may serve as an indicator of potential emergence of delirium and related symptoms such as agitation, or may be due to progression of illness. Cognitive decline, behavioral changes, and withdrawal have also been correlated with the pathogenesis of the delirious state. Duppils and Wikblad[28] noted several behavioral and psychological changes, such as anxiety, experienced in postoperative, elderly patients who subsequently developed delirium. Bush and Bruera,[13] in their exploration of delirium, noted lack of focus and inattention, as well as other cognitive changes including altered perceptions. The cognitive decline and withdrawal revealed by caregivers in the current study add to these findings and suggest that subtle and nonspecific signs and symptoms that characterize the progression of delirium may be clinically significant.
Alterations in the sleep/wake cycle have long been associated with delirium. The delirious state is known to include symptoms of daytime somnolence and reversal of the sleep/wake cycle as well as sleep interrupted by agitation and restlessness.[29,30] It remains uncertain whether a disrupted sleep cycle is a cause or consequence of delirium. A recent prospective, longitudinal study of 105 hospice patients found that poor sleep quality precedes delirium onset, adding support to a causal relationship between sleep disturbance and delirium.[31] Others have proposed a link between severe rapid eye movement deficiency and the development of delirium in neurodegenerative disease[31,32] as well as in intensive care unit patients.[33,34] The current findings describe a prodromal pattern of poor sleep quality progressing to fragmentation of the sleep/wake cycle, agitation, and cognitive disturbances. Although an orderly progression is suggested, the time period of sleep disturbance described in this study varied. However, recognition of the core deficit of sleep dysfunction may help alert clinicians and other members of the interdisciplinary team caring for the patient to the early signs of delirium or predelirious states.
The overarching theme reported by caregivers of delirious patients in this study was suffering. Clinicians share an understanding that delirium involves sufferable states, including pain, which are challenging to define.[33] In the current study, participants stated both indirectly and directly that they also experienced suffering as they witnessed the loss of personhood, which characterizes delirium. Suffering was also associated with each of the other categories of delirium-associated changes as well. There is an element of suffering associated with physical and cognitive decline, as well as patient withdrawal from loved ones, activities, and interests. Given complications such as nocturnal agitation and sleeplessness, it is not surprising that the interviews conducted in this study suggested that deteriorating sleep plays a key role in contributing to overall suffering for both patients and their caregivers. Previous research has also shown that caregivers may score even higher than their delirious loved ones on measures of distress leading to challenges in coping with consequences of delirium.[2]
Processing impending death is intrinsic to end-of-life closure and acceptance. However, this process also contributes to the spiritual and psychological suffering experienced by dying patients and their loved ones. Participants in this study consistently reported distressing comments made by their loved ones, which were categorized in this study as "end-of-life awareness." It is unclear to what extent the degree of distress associated with end-of-life awareness in this study was affected by developing delirium. The overall prevalence of suffering in the current study leads to questions regarding the relationship between confusional states and the psychological processing inherent to the dying process. Is it possible, for example, that the process of dying is associated with psychological discomfort that may also lower the threshold for delirium? Do states of severe psychological suffering contribute to the development of cognitive disorganization? Further research is needed to explore the association between end-of-life awareness, associated psychogenic distress, and the development of delirium.
Implications for Practice and Future Research
The current study highlights the importance of caregivers as witnesses to the signs and symptoms associated with the progression of delirium. Although delirium is common and distressing for end-of-life patients, the pathogenesis of delirium is poorly understood, and there is a clear need for caregiver education. Interviews of families whose loved ones experienced delirium at the end of life have demonstrated a desire for improved delirium screening and management.[21] Others have reported that families can assist in the prevention of delirium given their bedside presence and advocacy.[35] The current study suggests the existence of a set of signs and symptoms that may precede delirium and that may progress in a more or less predictable fashion to full-blown delirium. Findings from this research study are important for clinical practice, education, and research. An understanding of this progression may help lead to improved screening methods to identify delirium in its early, more easily treated stages, resulting in greater quality of life and a decrease in suffering for patients and their caregivers. A greater awareness of the prodromal symptoms of delirium may also help other members of the hospice interdisciplinary team, such as chaplains, social workers, aides, therapists, and even volunteers, identify patients at risk for development of delirium so that the patient's nurse and physician can intervene to provide education and intervention at earlier stages.Despite these limitations, the results of this study provide a starting point for future studies of the signs and symptoms of the prodrome to delirium and may help lead to earlier identification of and screening for delirium.
No comments:
Post a Comment