Making the Case for Palliative Care
April 29, 2013


The role of
palliative care is distinct from that of oncology, but the entities are
complementary. Determining the best ways to integrate these two types
of care is paramount to optimizing patient outcomes.
Throughout the United States,
palliative care (PC) is becoming a more established and integral
component of comprehensive cancer care for patients with advanced
disease. “Published research has shown that PC is associated with better
quality of life and mood, improved symptom control, and more
appropriate health resource use,” explains Jennifer S. Temel, MD. “It
has also been linked to increased patient and caregiver satisfaction,
healthcare savings, and survival.”
Clinical guidelines recommend that all
patients with metastatic cancer be offered PC services early in the
course of the disease. Currently, many cancer centers have some form of
PC services, such as inpatient consultative services and acute inpatient
units. PC clinics, on the other hand, are scarcer entities. Recent
analyses have suggested that integrating PC early in the ambulatory care
setting is feasible and can improve patient-reported outcomes as well
as several key measures of quality end-of-life care and resource use.
Early integration of PC with cancer care improves patients’
understanding of their disease and prognosis, leads to more timely
transitions to hospice care, and decreases chemotherapy use near the end
of life.
Looking Closer at Early Palliative Care
According to Dr. Temel, more information
about the nature and elements of early PC in ambulatory care is needed.
“The integration of PC with standard oncologic care may have a different
emphasis and focus than traditional inpatient or consultative PC,” she
says. Earlier and longer collaborative relationships between PC
clinicians and patients may allow the time and opportunity to face
complex issues like treatment decisions and advanced care planning
rather than focus mostly on acute symptom management and imminent death.
A study by Dr. Temel and colleagues published in JAMA Internal Medicine looked
at the content of clinic visits of early integrated PC in patients with
metastatic non–small cell lung cancer (NSCLC). The analysis involved 20
NSCLC patients who received early PC and survived less than 3 months, 3
to 6 months, 6 months to a year, and 1 to 2 years (five patients in
each group). A content analysis on PC and oncologic visit notes was
performed using electronic health records of participants. “Our intent
was to provide a framework for PC clinicians and oncologists to use in
developing integrated models of care at their institutions,” Dr. Temel
says.
Key Distinctions: Psychosocial Elements
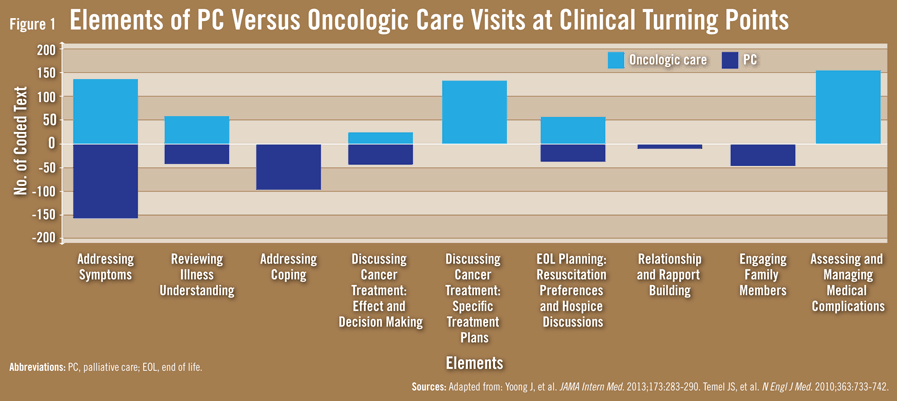
According to the study results, the role of
palliative care is distinct from that of oncology, but the entities are
complementary. Addressing symptoms and coping were the most prevalent
components of PC clinic visits (Figure 1).
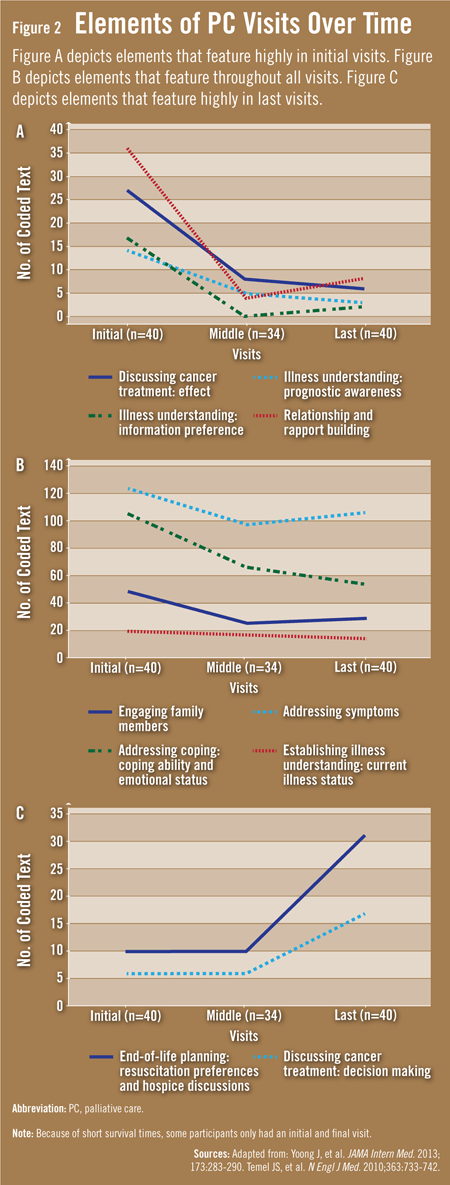
Initial visits focused on building relationships and rapport with
patients and families and on understanding the disease. Discussions
about resuscitation preferences and hospice occurred during later
visits. When comparing PC and oncologic care visits around critical time
points, both included discussions about symptoms and illness status (Figure 2).
However, PC visits tended to emphasize psychosocial elements (eg,
coping), while oncologic care visits focused on cancer treatment and
medical complications.
An interesting finding was that discussions
about end-of-life care occurred later in the course of illness. “Some
clinicians and patients still fear that PC will focus only on ‘death and
dying,’” Dr. Temel says. “Others believe it’s akin to going to hospice
care. Our study, however, confirms that PC focuses on supporting
patients and families as they navigate their diagnosis. PC isn’t solely
focused on end-of-life care.”
A Roadmap to Integrated Palliative Care
The study by Dr. Temel and colleagues sheds
light on the clinical components of early integrated PC in ambulatory
care. “Our hope is that this can serve as a roadmap or guide for PC
clinicians who are developing outpatient services for patients with
newly diagnosed advanced cancer or other illnesses,” says Dr. Temel.
“The expertise from a collaborative clinical team can enable and provide
adequate time for oncologists to focus on cancer therapy and medical
management of the disease.”
As integrated PC and oncologic care becomes
more widely accepted and available, there may be important implications
for oncology training. “Each institution will need to develop training
protocols to optimize approaches to adopting early PC,” Dr. Temel says.
“With more research, it’s hoped that we’ll be able to determine if the
benefits of early integrated PC can be generalized and find components
of our intervention that are most effective.”
Additional Resources:
Yoong J, Park ER, Greer JA, et al. Early palliative care in advanced lung cancer: a qualitative study. JAMA Intern Med. 2013 Jan 28 [Epub ahead of print]. Available at: http://archinte.jamanetwork.com/article.aspx?articleid=1566605.
Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med. 2010;363:733-742.
Smith TJ, Temin S, Alesi ER, et al. American
Society of Clinical Oncology provisional clinical opinion: the
integration of palliative care into standard oncology care. J Clin Oncol. 2012;30:880-887.
Bruera E, Hui D. Integrating supportive and palliative care in the trajectory of cancer: establishing goals and models of care. J Clin Oncol. 2010;28:4013-4017.
Ferris FD, Bruera E, Cherny N, et al. Palliative cancer care a decade later: accomplishments, the need, next steps: from the American Society of Clinical Oncology. J Clin Oncol. 2009;27:3052-3058.
Walling A, Lorenz KA, Dy SM, et al. Evidence-based recommendations for information and care planning in cancer care. J Clin Oncol. 2008;26:3896-3902.
Kamal AH, Bull J, Kavalieratos D, et al. Palliative care needs of patients with cancer living in the community. J Oncol Pract. 2011;7:382-388.
Rabow MW, Smith AK, Braun JL, Weissman DE. Outpatient palliative care practices. Arch Intern Med. 2010;170:654-655.
Jacobsen J, Jackson V, Dahlin C, et al. Components of early outpatient palliative care consultation in patients with metastatic nonsmall cell lung cancer. J Palliat Med. 2011;14:459-464.
Barnes KA, Barlow CA, Harrington J, et al. Advance care planning discussions in advanced cancer: analysis of dialogues between patients and care planning mediators. Palliat Support Care. 2011;9:73-79.
No comments:
Post a Comment